When we evaluate whether a rehabilitation intervention works, we instinctively ask: “Does it improve outcomes?” But this question, while seemingly straightforward, reflects a fundamental misunderstanding about how rehabilitation works and what determines patient outcomes.
Outcomes are not simply the output of treatments.
Unlike taking a pill that biochemically alters physiology, rehabilitation operates within a complex system involving the patient’s biology, psychology, social context, environment, healthcare system, and broader societal factors. The rehabilitation intervention is just one element—often not even the most important one—in determining whether someone recovers function, returns to work, or maintains independence.
This post explores what really determines rehabilitation outcomes, why the biomedical “treatment → outcome” model is insufficient, and how we can better understand and measure success in rehabilitation.
The Problem with the Linear Treatment Model
Traditional clinical research operates on a simple premise:
Treatment → Outcome
Give intervention X, measure outcome Y, compare to control. If Y improves more with X than without X, the treatment works.
This model works reasonably well for some medical interventions:
- Antibiotics kill bacteria → infection resolves
- Insulin lowers glucose → prevents diabetic complications
- Anticoagulants prevent clots → reduce stroke in atrial fibrillation
Even here, the model is oversimplified—patient adherence, access to care, comorbidities, and social determinants all matter. But for acute, biologically-driven interventions, the approximation is useful.
In rehabilitation, this model fundamentally breaks down.
Rehabilitation outcomes are not simply the product of what therapists do in treatment sessions. They emerge from the complex interaction of:
- Person factors: Severity of impairment, comorbidities, age, cognition, motivation, self-efficacy, coping strategies, mental health, prior experiences, genetics
- Intervention factors: Type, intensity, duration, timing, quality, therapist expertise, therapeutic relationship
- Environmental factors: Physical environment, assistive technology, home modifications, accessibility, workplace accommodations
- Social factors: Family support, social networks, caregiver availability, cultural beliefs, socioeconomic status, health literacy
- System factors: Healthcare access, insurance coverage, wait times, care coordination, continuity, interdisciplinary collaboration
- Societal factors: Policies, disability attitudes, employment laws, social safety nets, community resources
The rehabilitation intervention interacts with all of these factors—it doesn’t independently produce outcomes.
The ICF Framework: A Better Model for Understanding Rehabilitation Outcomes
The International Classification of Functioning, Disability and Health (ICF) provides a more sophisticated framework for understanding how outcomes are determined.
The ICF Model
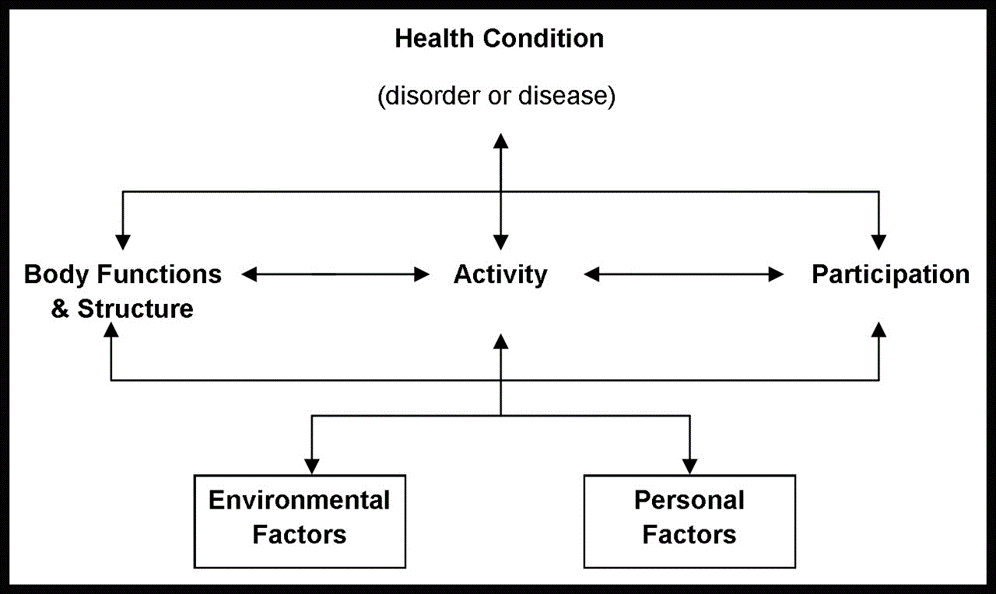
All of these are influenced bidirectionally by:
- Environmental Factors (barriers and facilitators)
- Personal Factors (individual attributes and life circumstances)
What This Means for Rehabilitation Outcomes
Outcomes occur at multiple levels:
- Body structure/function: Range of motion, strength, balance, pain, cognition
- Activity: Walking, dressing, cooking, managing medications
- Participation: Working, socialising, hobbies, community engagement
- Quality of life: Well-being, life satisfaction, psychological health
Critical insight: An intervention might improve body function without improving activity. It might improve activity without improving participation. It might improve all three, but not the quality of life.
Why? Because outcomes at each level are influenced by different factors:
- Improved knee range of motion (body function) doesn’t guarantee improved walking (activity) if the person lacks confidence, has poor balance, or lives in an inaccessible environment
- Improved walking ability (activity) doesn’t guarantee return to work (participation) if the workplace is inaccessible, the employer discriminates, or transportation is unavailable
- Return to work (participation) doesn’t guarantee quality of life if the person experiences chronic pain, social isolation, or financial stress
The intervention is necessary but not sufficient for meaningful outcomes.
Ultimately, rehabilitation outcomes should not be understood as simple reflections of whether a treatment “worked.” They are shaped by a dynamic interaction between the intervention, the individual receiving it, the environment in which recovery occurs, and the wider systems that support—or constrain—progress. If rehabilitation is to be understood, delivered, and evaluated more meaningfully, we must move beyond narrow treatment-effect thinking and adopt a broader, person- and context-sensitive view of outcome. In rehabilitation, success is rarely the product of a single intervention; it is the result of how care, capacity, context, and lived experience come together over time.
Thanks for Reading!
Ammar Suhail

Leave a comment