A few years ago, we wrote a blog post about why we started researching back pain. You can read it here. In it, we described our early confusion as clinicians, our introduction to Evidence-Based Practice, and the first set of studies we embarked on to understand the beliefs and myths surrounding low back pain in India.
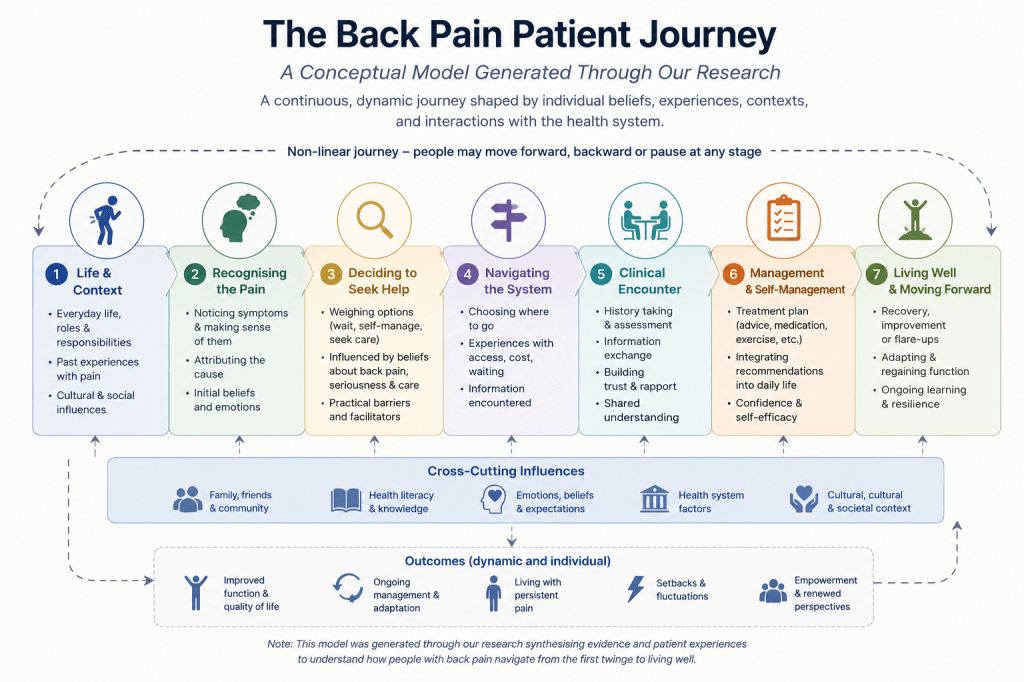
Since then, our research has grown. We have published more studies, added new questions, and perhaps most importantly, developed a clearer sense of how all of this work connects. We wanted to update that original blog to reflect where we are now. But rather than simply adding new papers to the list, we thought it would be more useful to organise everything around a concept that has been quietly shaping our thinking all along: the patient journey.
What we mean by that is that every person who comes to a physiotherapist with back pain has travelled a path to get there. The path people take is influenced by what they read, what they are told, their beliefs about their body, and the type of clinician and advice they encounter when they finally seek help. Our research has, piece by piece, been mapping different points along that path. This blog is our attempt to show how those pieces fit together, and to be honest about where the gaps still are, gaps that our ongoing and future research is working to fill.
So here is our updated understanding, told through the lens of a patient journey.
The Patient Who Walked In
To understand why our research matters, it helps to think about a single patient. Let us call her Priya. She is 34 years old, has had low back pain for three weeks, and has come to see a physiotherapist. Before she even sits down, something important has already happened: she has already formed beliefs about her pain. She has read a few websites. She has spoken to her mother, who had the same problem and never fully recovered. She has been resting, because she read that movement might cause damage.
Priya’s story is not unusual. It is, in fact, the norm. And our research studies have been, in many ways, a systematic attempt to understand everything that has gone wrong before she arrived and what needs to change so that her care actually helps her.
Before Priya Arrives: The Information Problem
The first thing worth understanding is where Priya’s beliefs came from. Most people with back pain turn to the internet before they see a clinician. Research suggests that approximately half of patients with low back pain search the internet for health and medical advice, often before or alongside consulting a clinician. We wanted to know what they find there.
In our content analysis of online information about back pain (Suhail & Quais, 2022), we screened the top results returned by Google for searches like “low back pain,” “back pain,” and “backache.” A total of 53 websites were included. What we found was consistent and concerning: the information available online did not reflect evidence-based guidelines. Websites consistently presented a structural, biomedical picture of back pain, focusing on anatomical causes, imaging, and passive treatments. The nuance of the biopsychosocial model, which acknowledges that pain is shaped by biological, psychological, and social factors together, was largely absent.
So when Priya reads that her pain is caused by a “weak core” or “poor posture,” she is not misreading the internet. The internet is telling her exactly that.
In a companion opinion paper (Suhail & Poulter, 2022), we mapped out the broader sources through which people acquire their beliefs about back pain. These include media, informal conversations, family history, and online content — all of which tend to transmit the same biomedical narrative. This means that by the time a patient like Priya walks into a clinic, she has been receiving a consistent, if inaccurate, message about her spine for years.
When we conducted that content analysis, the dominant concern was websites. But the information landscape has shifted considerably since then. Increasingly, people are not just searching Google; they are asking AI. Tools like ChatGPT, Gemini, and others have become a first port of call for health questions, including questions about back pain. For many people, AI feels more accessible and more conversational than reading through a list of search results. The concern, of course, is whether the information these tools generate is any more accurate or helpful than what we found on those websites.
This is a question we are actively working to answer. We are currently exploring whether AI-generated responses to common back pain queries reflect current evidence-based guidelines, or whether they reproduce the same biomedical narrative that we found so pervasive online. It is an emerging and important piece of the information problem, because if Priya is now asking an AI chatbot about her back before she sees a clinician, we need to understand what that chatbot is telling her. We will share findings as that work develops.
What Priya Believes: The Myth Problem
We explored what these beliefs actually look like in practice. In our first study (Suhail, Slathia, Quais & Poulter, 2021), we surveyed young college-going adults in India with a history of low back pain. We used a validated questionnaire based on Deyo’s “Myths of Back Pain” and an editorial by O’Sullivan and colleagues. The findings were striking. Myths about back pain were widespread. People believed that poor posture causes LBP, that their pain would worsen with age, that a scan was necessary, and that exercise during pain meant damage was being done.
These are not harmless misunderstandings. The literature is clear that these beliefs — particularly catastrophising and fear of movement are among the strongest predictors of pain becoming chronic. When Priya tells her physiotherapist, “I’ve been resting because I’m scared of making it worse,” she is not being irrational. She is acting on what she has been told by sources she has every reason to trust.
The Clinician in the Room: The Training Problem
Here is where the story becomes more uncomfortable. The problem is not only in what patients believe. It is also in what clinicians believe.
We explored this in two studies focused on physiotherapy students. In our first student-focused study (Suhail & Quais, 2023), we surveyed 265 undergraduate physiotherapy students from institutions across northern India. We found that myths about LBP were widely held among them — in some cases, more widely than we had expected. The most prevalent myth, endorsed by 94.7% of students, was that LBP is caused by poor posture when sitting, standing, or lifting. The belief that weak core muscles cause back pain and that a strong core protects against future LBP was endorsed by 87.5%. The belief that LBP will become persistent and deteriorate in later life was held by 83.4%.
These students were not in their first week of training. Some differences emerged across academic years. Students in their third and fourth years were less likely to believe that surgery was necessary for a slipped disc, and less likely to think strong medications or injections were essential. That is encouraging. But the foundational myths, the ones about posture, the core, and deterioration, persisted stubbornly across all four years of training.
We took this further in a more recent study (Suhail & Quais, 2025), using a validated scale called the Pain Attitudes and Beliefs Scale for Physiotherapists (PABS.PT). This time, we surveyed 445 students, comparing first-year and fourth-year students across institutions in North India. The findings were sobering. Students consistently scored higher on biomedical beliefs than on biopsychosocial beliefs, and this did not change meaningfully between the first and fourth years. The biopsychosocial scores were virtually identical across both groups (mean of 23.8 for both years). Four years of physiotherapy education did not shift how students fundamentally conceptualised pain.
We also found that having personal experience of back pain made no difference to belief orientation. Students who had themselves experienced LBP were no more likely to hold biopsychosocial beliefs than those who had not. This challenges the assumption that experiential learning through personal pain automatically produces more accurate or helpful beliefs. It suggests that beliefs are shaped more by what is taught — and how — than by what is felt.
What does this mean for Priya? It means that the physiotherapist she is seeing may well hold many of the same unhelpful beliefs about back pain that she does. And as the literature consistently shows, the beliefs of clinicians shape the advice and information they give to patients. The words a physiotherapist chooses in that first appointment can either reinforce Priya’s fears or begin to gently challenge them.
What the Evidence Actually Looks Like: The Research Quality Problem
Even when a clinician wants to follow the evidence, what evidence is available to them — at least in the Indian context?
We examined this in a systematic review of clinical trials on LBP conducted by Indian physiotherapists (Quais & Suhail, 2024). We searched MEDLINE and the PEDro database for eligible trials published between 2005 and 2021. Of 866 records screened, 37 studies were included for final analysis.
The methodological quality of these trials, assessed using the PEDro scale, ranged from poor to fair, with a mean score of 5.17 out of 10. Only one study was rated as excellent. Among the most common problems: 83.7% of studies did not report a sample size calculation, only 10.8% had prospective trial registrations, and the vast majority did not include long-term follow-up. Most trials measured only short-term or immediate outcomes, which tells a clinician relatively little about how to support a patient like Priya over weeks and months.
There was also a striking lack of diversity in the interventions being studied. The majority of trials focused on core strengthening or manual therapy, precisely the interventions most tied to the biomedical narrative that our earlier studies found so pervasive. Research on psychosocial interventions, pain neuroscience education, or patient-centred approaches was sparse.
This creates a difficult situation. A clinician trained in a biomedical paradigm, consulting an evidence base that overwhelmingly reflects that same paradigm, is unlikely to offer Priya the kind of care that current international guidelines actually recommend.
What Priya Deserves
When Priya finally sits down across from her physiotherapist, she deserves a clinician who can do several things at once.
She deserves someone who understands that her beliefs about her back (the posture narrative, the fear of deterioration, the instinct to rest) did not come from nowhere. They came from her family, from the websites she read, and quite possibly from healthcare encounters she has had before. Our research has tried to map exactly where those beliefs originate and how widely they are held, because you cannot change something you have not first understood.
She deserves someone who has themselves been trained in a way that moves beyond the structural, biomedical model. Our studies suggest that four years of physiotherapy education in India is not currently sufficient to achieve this shift. That is not a criticism of students or of educators — it is a finding that points toward what needs to change in curricula. Integrating pain neuroscience education, reflective practice, and biopsychosocial frameworks early and consistently into training programmes is not an add-on. It is, based on our findings, an urgent priority.
And she deserves care that is grounded in high-quality, contextually relevant evidence. The trials that have been conducted by Indian physiotherapists are an important beginning, but there is significant room for improvement in how those trials are designed, registered, and reported. Future research needs to move beyond short-term outcomes, diversify the interventions it examines, and meet the methodological standards that would allow its findings to be trusted.
Where the Gaps Are — and Where We Are Going
Mapping our research onto the patient journey has helped us see not only what we have done, but what remains to be done. The journey has at least three points where the evidence is still thin.
The first is the general population. We know what college-going adults and physiotherapy students believe about back pain in India. But the broader public — people who are not in higher education, who live in rural areas, who access care through very different channels remains largely unstudied. We are currently completing data collection on this study, and it is a gap that matters because Priya is more likely to come from that population than from a university campus.
The second is the practising clinician. Our student studies tell us what beliefs look like before training is complete. But what do qualified, practising physiotherapists in India actually believe about back pain, and how do those beliefs translate into what they say and do in a clinic?
The third is the intervention. Understanding the problem is only half the work. What actually shifts beliefs — in students, in clinicians, in patients? What does a curriculum intervention look like that genuinely moves the needle on biomedical thinking? These are the questions that sit downstream of everything we have published so far, and they are the ones we are working towards.
The patient journey framework has given us a way to see all of this together. Priya’s experience of back pain is shaped at every point by what she reads online, by what her family tells her, by what her clinician believes, and by the quality of the evidence that clinician draws on. Our research has touched each of those points. The work ahead is to connect them more deliberately and to start asking not just what is wrong, but what would actually make it better.
We will keep writing as the work develops. Follow the blog for updates.
Thanks for Reading!
Ammar Suhail
References
Suhail, A., Slathia, S., Quais, S., & Poulter, D.C. (2021). Do “Myths” of low back pain exist among young Indian college-going adults with a history of low back pain? A cross-sectional study. Bulletin of Faculty of Physical Therapy, 26, https://doi.org/10.1186/s43161-021-00036-w
Suhail, A., & Quais, S. (2023). Do undergraduate physiotherapy students believe back pain myths? A cross-sectional survey. Journal of Rehabilitation Sciences and Research, 10(1), 38–43. https://jrsr.sums.ac.ir/article_48475.html
Suhail, A., & Poulter, D.C. (2022). Where do people acquire their beliefs about low back pain? International Journal of Osteopathic Medicine, 45, 38–40. https://doi.org/10.1016/j.ijosm.2022.06.004
Suhail, A., & Quais, S. (2022). Content analysis of the online information available about back pain. Bulletin of Faculty of Physical Therapy, 27, 23. https://doi.org/10.1186/s43161-022-00081-zQuais, S., & Suhail, A. (2024).
Quality and quantity of clinical trials on low back pain published by Indian physiotherapists. Bulletin of Faculty of Physical Therapy, 29, 14. https://doi.org/10.1186/s43161-024-00185-8
Suhail, A., & Quais, S. (2025). Low back pain belief orientations among undergraduate physiotherapy students: A cross-sectional study. Musculoskeletal Care, 23, e70167. https://doi.org/10.1002/msc.70167

Leave a comment