The International Classification of Functioning, Disability and Health (ICF) is a framework developed by the World Health Organisation to help healthcare professionals understand health beyond a diagnosis. Rather than focusing only on disease or injury, the ICF considers how a person’s health condition affects their daily activities, participation in society, and overall quality of life.
The framework recognises that health is influenced not only by physical impairments but also by personal and environmental factors. By providing a common language to describe functioning, the ICF helps clinicians communicate more effectively, set meaningful goals, and deliver person-centred care.
This blog introduces the key components of the ICF and explores how it can be applied in everyday clinical practice.
Why was the ICF Developed?
Traditionally, health conditions were often described primarily in terms of diagnosis, disease, or impairment. While these aspects are important, they do not always capture how a condition affects a person’s daily life. Two individuals with the same diagnosis may experience very different levels of functioning, participation, and quality of life.
To address this gap, the World Health Organisation (WHO) developed the International Classification of Functioning, Disability and Health (ICF) in 2001. The ICF provides a biopsychosocial framework that integrates medical and social perspectives of health. It recognises that disability and functioning arise from the interaction between a person’s health condition and contextual factors, including their environment and personal circumstances.
By focusing on functioning rather than diagnosis alone, the ICF helps healthcare professionals understand the full impact of a health condition and supports more comprehensive, person-centred care.
The Components of the ICF
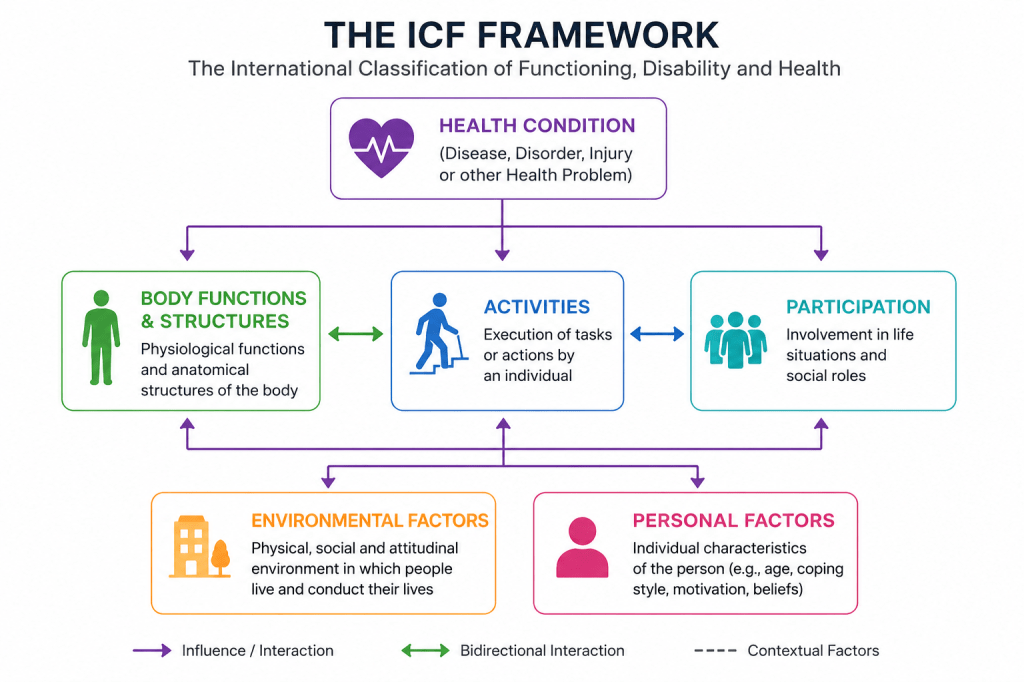
The ICF views health and disability as the result of interactions between a health condition and various contextual factors. Rather than focusing solely on a diagnosis, it considers how a person’s body functions, daily activities, participation in society, and surrounding environment influence their overall functioning.
Figure 1. The International Classification of Functioning, Disability and Health (ICF) Framework
Why Use the ICF in Clinical Practice?
1. Keeps the Patient at the Centre
- Focuses on the person, not just the diagnosis.
- Captures what patients can do, cannot do, and what matters most to them.
- Supports patient-centred goal setting.
2. Makes Clinical Reasoning Clear
- Links impairments to activity limitations and participation restrictions.
- Provides a clear rationale for treatment decisions.
- Makes documentation easier to understand and review.
3. Improves Team Communication
- Creates a common language across healthcare professions.
- Enhances referrals, handovers, and multidisciplinary collaboration.
- Reduces misunderstandings between providers.
4. Supports Meaningful Outcomes
- Measures changes in function, activities, and participation.
- Demonstrates the real-world impact of physiotherapy.
- Helps show the value of rehabilitation services.
5. Enhances Documentation Quality
- Promotes structured and consistent record-keeping.
- Improves continuity of care.
- Makes clinical notes more transparent and reproducible.
In essence, the ICF helps physiotherapists move beyond diagnosing problems to understanding how those problems affect a person’s daily life and participation in society.
A worked example — step by step
The following case illustrates how to build an ICF-structured assessment for a patient you might see any day of the week

Begin with the patient’s perspective — activities and participation
Before your formal examination, ask open questions about what the patient can no longer do. This is where the ICF connects with patient-centred care — mapping life impact, not just symptoms.
“What can you not do now that you could before the pain started?”
Sarah: “I can’t sit at my desk for more than 20 minutes, I can’t stand up in front of the class all morning, and I’ve stopped going for my evening walks.”
“What does a normal day look like for you right now?”
Sarah: “I spend most of it on the sofa. I can’t sleep properly because of the pain at night. I feel useless — I haven’t been able to teach for four months.”
Map what you hear to the ICF domains
Translate the patient’s words into the three ICF functioning domains (PATIENT SAYS → ICF DOMAIN). You don’t need to memorise codes — a reference sheet or the WHO ICF browser handles that. The thinking is what matters.
“Can’t sit more than 20 minutes”
Activity limitation — maintaining a body position d415
“Can’t stand in front of the class”
Participation restriction — remunerative employment d850
“Stopped evening walks”
Participation restriction — recreation and leisure d920
“Can’t sleep because of pain”
Activity limitation — sleeping d710 / Body function — sleep functions b134
Conduct your examination — map findings to body functions
Physical examination findings map to body functions and structures — the impairments that are hypothetically driving the activity limitations and participation restrictions identified above (CLINICAL FINDING → ICF CODE)
Reduced lumbar flexion range, pain on overpressure →Reduced mobility of joint functions b710
Hip abductor weakness (4-/5 bilaterally) →Reduced muscle power function b730
Central low back pain, NRS 6/10 at rest, 8/10 with sitting →Sensation of pain b280
Identify contextual factors
Environmental and personal factors can either facilitate recovery or act as barriers. In Sarah’s case, some important ones emerge during conversation.
PERSONAL FACTORS
“I’m frightened to move in case I make it worse.”
Fear-avoidance beliefs — a personal contextual factor likely amplifying activity limitations beyond what the physical impairment alone would explain. This should shape the treatment approach (graded exposure, pain education).
ENVIRONMENTAL FACTORS
School has no adjustable-height desks. Sarah has a supportive GP and an understanding headteacher.
Barrier: design of school environment e155.
Facilitator: health professionals e355and attitudes of people in authority e430.
Compile the ICF table — your structured case documentation
Bring everything together into the standard ICF structure. This becomes your case notes, your referral letter, or your case report.
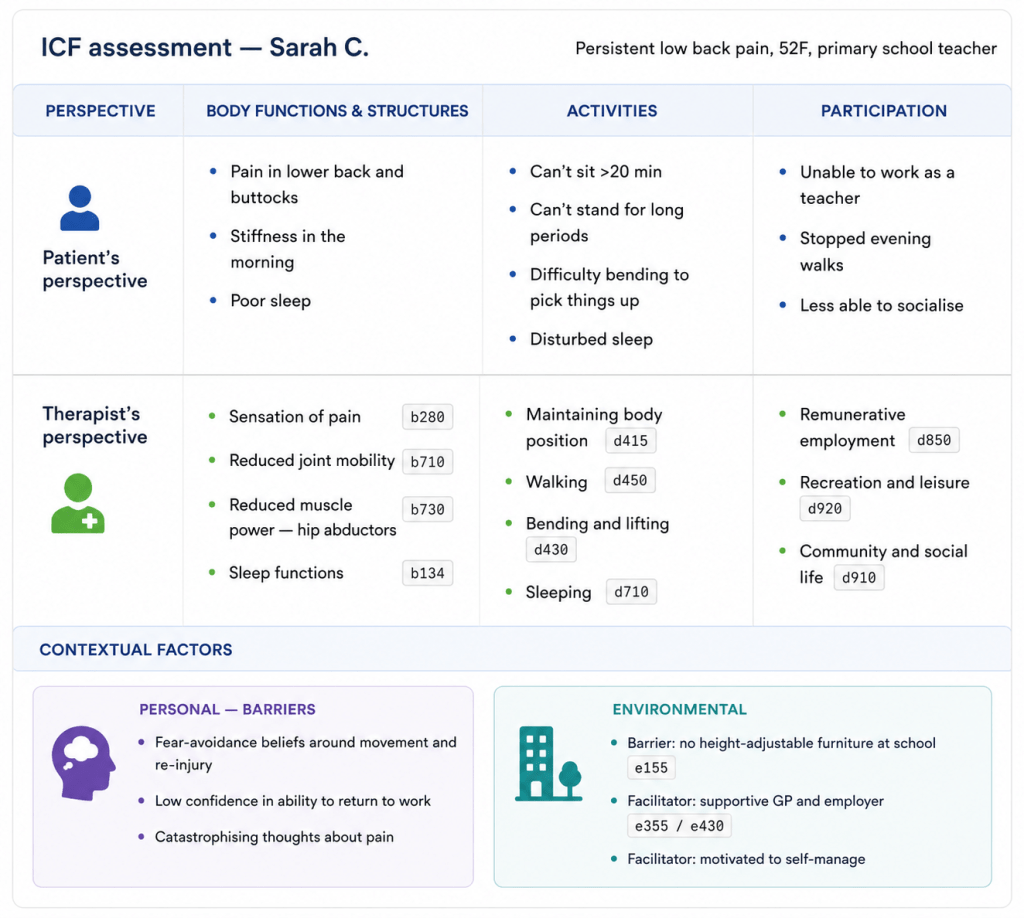
This table shows what a standard SOAP note often cannot: the reasoning chain connecting hip weakness (b730) to sitting tolerance (d415) to inability to work (d850), and flags that fear-avoidance beliefs need addressing alongside physical impairments — otherwise treatment gains are likely to plateau. That reasoning is now legible to every clinician who reads this file.
Key Takeaways
It reflects existing practice
- The ICF formalises clinical thinking you already have.
- No new assessments needed — just a structured way to record what you find.
Start with “what can’t you do?”
- Activity limitations and participation restrictions are the heart of physiotherapy.
- Begin there, then work backwards to body functions.
Contextual factors matter
- Fear-avoidance, workplace barriers, family support — these often explain why two patients with identical impairments have very different outcomes.
Bringing the ICF into Practice
The example presented above illustrates one way the ICF can be used to organise clinical information. Separating the patient’s perspective from the therapist’s perspective can help ensure that both lived experiences and clinical findings are captured during assessment. While the patient’s perspective highlights the challenges that matter most to the individual, the therapist’s perspective allows these concerns to be linked to specific domains of functioning within the ICF framework.
Similarly, documenting personal and environmental factors helps place a person’s difficulties within their broader context. Factors such as beliefs, motivation, family support, workplace demands, and access to resources can all influence recovery and participation. Recording these factors alongside impairments and activity limitations can provide a more complete picture of the individual’s situation.
The format shown here is only one example, and clinicians may adapt it to suit their own practice settings. Whether used for assessment, goal setting, documentation, or communication with other healthcare professionals, the ICF offers a structured way to organise information and maintain a focus on what matters most to the person receiving care.
Ultimately, the value of the ICF lies not in the framework itself, but in its ability to help clinicians understand patients more comprehensively and support meaningful improvements in functioning, participation, and quality of life.

Leave a comment